

A System at Breaking Point: What Privatisation Means for Patients, Staff and the Future of Mental Health Care (NHS Privitisation Part 3)
How outsourcing, understaffing and market logic are fragmenting mental health care - and why the damage may already be irreversible.
Dr. John Mulligan
Privatisation rarely announces itself. It doesn’t arrive with the drama of a ministerial statement or a sweeping legislative change. Instead, it emerges through a slow and deliberate erosion: the closure of a day unit, the outsourcing of a specialist service, the quiet rewriting of commissioning frameworks to make private providers not just optional, but inevitable. And when mental health care is already fragile - skeletal teams, high turnover, exhausted staff - these pressures don’t simply reshape the system. They break it.
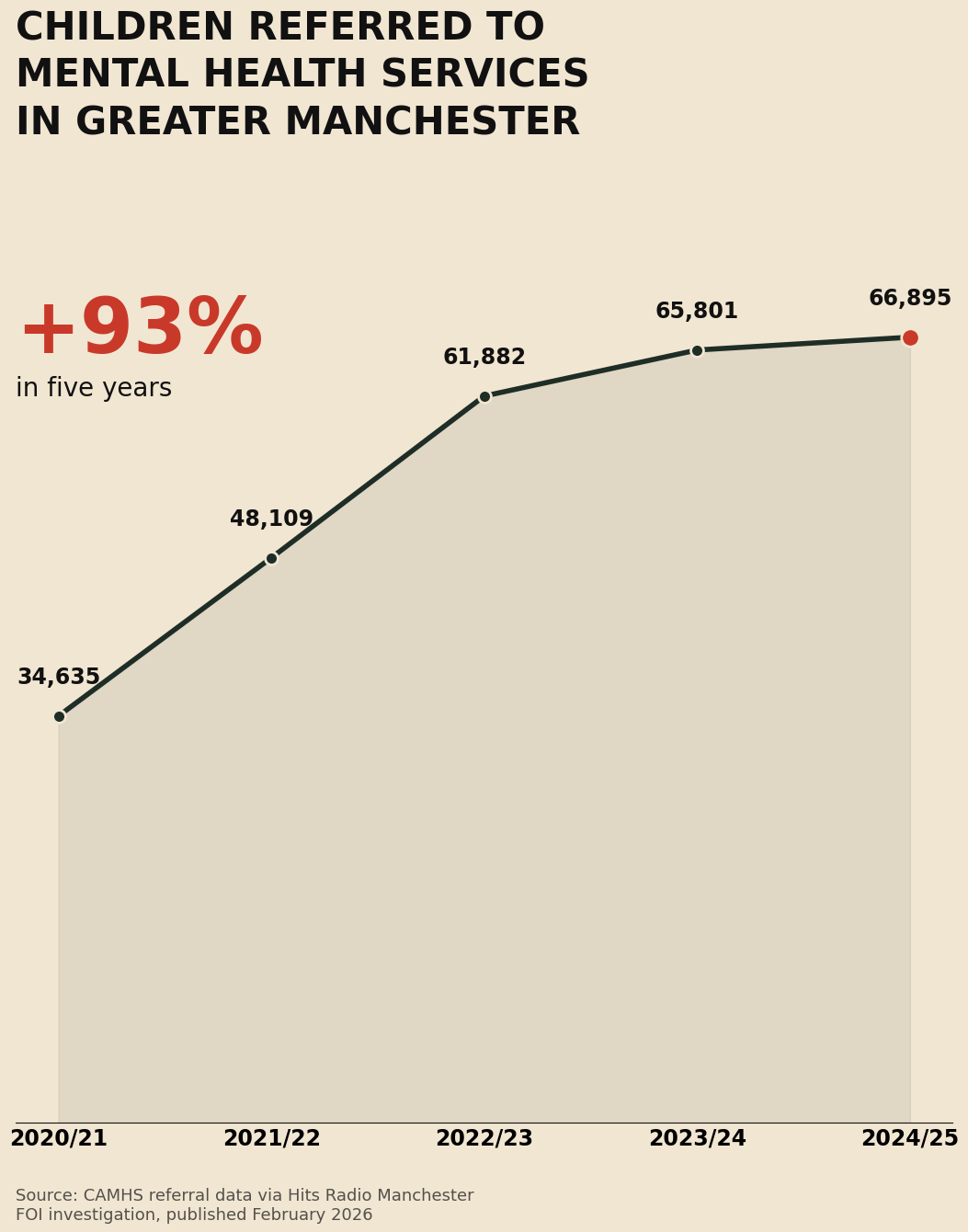
Across England, NHS community mental health teams are buckling under decades of neglect. Workforce shortages that were once described as “concerning” are now terminal. Staff are spread so thinly that continuity of care - the foundation of safe mental health practice - has become a luxury, not a standard. At the same time, private companies and large VCSEs are absorbing bigger and bigger portions of public money, often delivering worse outcomes at far higher cost. The public is told services remain “free at the point of use,” as though that phrase alone can protect against everything happening beneath the surface.
This article looks at what privatisation is already doing to the workforce, to patient care, and to the future of the NHS itself - and why we need an urgent parliamentary debate before the damage becomes irreversible.
The Workforce Is the Heart of Mental Health Care - and It Is Being Hollowed Out
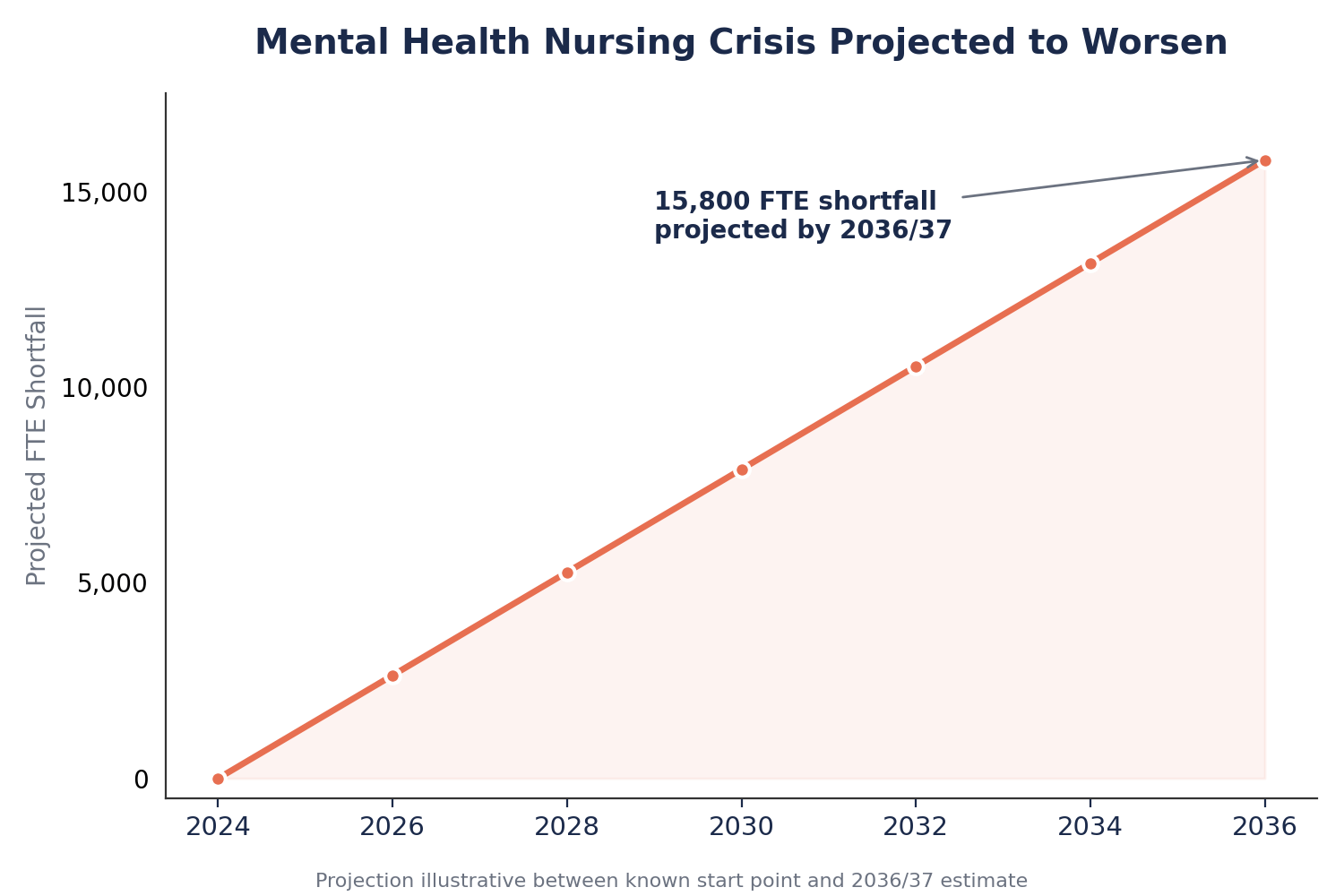
Mental health care relies on expertise: psychiatrists, psychologists, nurses, OTs, social workers, peer workers, support staff, administrators. When you weaken that workforce, you weaken everything else. But national workforce planning has been repeatedly delayed, watered down or quietly abandoned - largely because publishing the numbers would expose the scale of political failure.
The result is a system where:
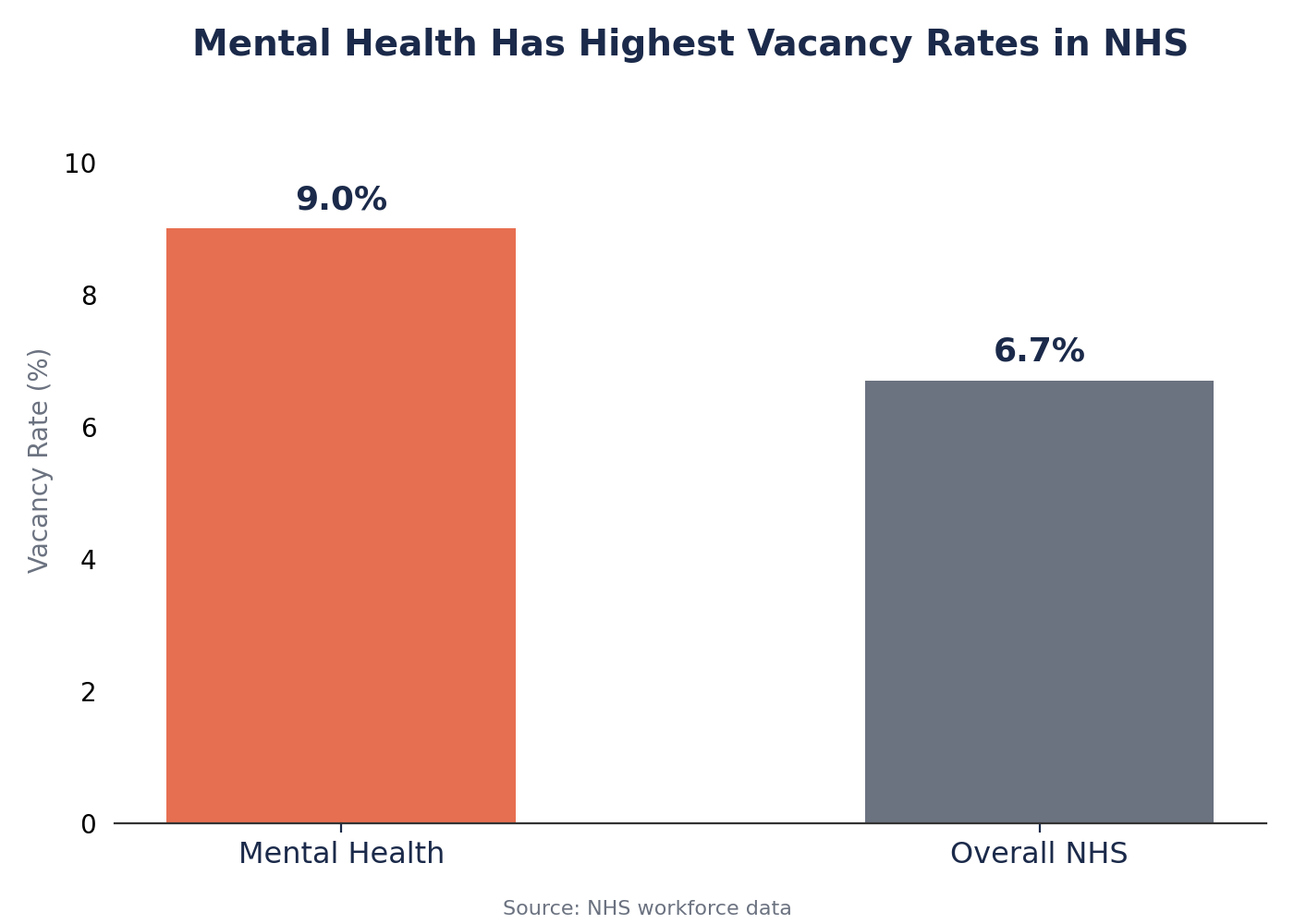
· Vacancies remain open for months or even years
· Teams operate at 40–60% of required staffing
· Newly qualified staff are thrown into high-risk roles without support
· Experienced clinicians leave for better pay and safer working conditions
· “Skill-mixing” is used as a euphemism for diluting clinical expertise
In this context, the rise of private and VCSE contracts doesn’t relieve pressure - it intensifies it. Many of these organisations require NHS staff to move across to deliver services, draining teams already on their knees. Others operate with minimal qualifications, creating a parallel workforce with fewer protections and less training.
Patients do not receive a “choice” in this shift. They simply receive worse care.
Privatisation Doesn’t Need Fees at the Door - the Damage Happens Long Before That
Politicians often reassure the public that privatisation isn’t happening because the NHS remains free at the point of use. But privatisation doesn’t begin when you’re forced to pay. It begins when services are carved up, outsourced, fragmented and hollowed out - until the only providers left standing are private.
Here’s what that looks like on the ground:
1. Longer waiting times become normalised
When private or VCSE organisations fail to deliver, patients are sent back to the NHS - only now the NHS has even less capacity to absorb them.
2. Complex cases are left with NHS teams
Private providers often take on “light-touch” work with predictable outcomes, while NHS teams are left managing the most distressed, unwell and high-risk patients with the least resources.
3. Local knowledge evaporates
Mental health care is relational. Understanding housing associations, community networks, GP relationships, schools, crisis teams - this takes time. Private organisations often rotate staff, rely on short contracts, or simply don’t have this background.
4. Standards quietly fall
When commissioners outsource services to meet “transformation targets,” scrutiny decreases. Contracts are monitored on paper, not practice. Meanwhile, NHS staff are held to ever-tighter standards.
5. Money is spent on management, not care
Private and large VCSE providers absorb millions in “infrastructure,” “overheads,” “leadership teams,” and “innovation frameworks.” The NHS cannot compete with its own money being used against it.
This is privatisation - not in theory, but in lived experience.
The Long-Term Costs Are Catastrophic - Financially and Clinically
Privatisation is often sold as efficiency. In mental health, it has done the opposite.
Private inpatient beds are dramatically more expensive than NHS ones
Trusts now spend hundreds of millions annually sending patients to private hospitals. These beds frequently offer:
· Lower staffing levels
· Less experienced clinicians
· Higher rates of restraint
· Worse outcomes
But because NHS beds have been shut down, trusts have no alternative.
Community contracts are awarded to organisations with little expertise
Across England, “transformation” money has been funnelled into corporate-scale VCSEs and private companies to run highly complex services. These groups often:
· Deliver minimal clinical work
· Use unskilled staff
· Fail to meet targets
· Require major corrections by the NHS
The public ends up paying more for worse care.
Fragmented care is expensive care
When multiple organisations handle different fragments of a patient’s journey, communication fails. Patients bounce between services, relapsing, withdrawing, repeating assessments, and eventually entering crisis.
Crisis care is the most expensive form of care.
Fragmentation therefore isn’t just unsafe; it is financially irrational.
The Ideological Shift: Mental Health Care as a Marketplace
Underlying this entire process is an ideological shift: mental health care reimagined not as a public service, but as a market. Patients become “service users,” clinicians become “providers,” and care pathways become “products.” Contracts replace relationships. Procurement frameworks replace clinical reasoning.
This shift has real consequences:
· Clinical expertise is devalued
· Short-term contracts replace long-term investment
· Outsourcing becomes the default
· Commissioners are incentivised to choose the cheapest bidder, not the best service
· Patient needs become secondary to market logic
It is an approach that prioritises appearances - “transformation,” “innovation,” “community-led models” - over outcomes. It is an approach that asks: How cheaply can we do this? rather than What do patients need to stay well and alive?
Where This Leads If Unchallenged: A Dystopian Future Already Taking Shape
If current trends continue, mental health care in England could become a patchwork of inconsistent, semi-privatised services where:
· NHS community teams become small crisis-response hubs
· Most “care” is outsourced to low-paid, low-skilled providers
· Patients are triaged, assessed and signposted endlessly
· Private inpatient beds become the norm
· Standards vary wildly between areas
· Preventable deaths continue to rise
· Accountability becomes impossible
In such a future, “free at the point of use” becomes meaningless. Care that is technically free can still be unsafe, inadequate or dehumanising.
This is not speculation. It is the direction of travel.
Why We Need Parliamentary Scrutiny. Now.
The Early Intervention in Psychosis team going on strike is not an isolated event. NHS mental health staff are increasingly speaking out because they have reached the limit of what can be sustained safely or ethically.
We need:
· A full parliamentary debate on Community Transformation and privatisation
· A published national mental health workforce plan
· Transparency on where mental health budgets are going
· Evidence-based assessment of VCSE and private sector outcomes
· A commitment to rebuilding NHS services, not replacing them
For years, the deterioration of mental health care has been treated as an unfortunate inevitability. It is not. It is a political choice - one that can be reversed if there is public pressure and honest debate.
The stakes are too high for silence. The NHS can survive neglect for a while. It cannot survive being dismantled piece by piece while pretending everything remains the same.
